As a rule of thumb, overthinking and stressing about sleep is not a good thing to do, especially if you are prone to insomnia symptoms. It may sound contradictory since this website aims to raise awareness about the importance of sleep, sleep disorders and the health consequences of not having a good night’s sleep. However, there is a crucial difference between getting informed to take healthy decisions and worrying too much, being stressed or downright obsessed or frightened about a health matter. With insomnia especially, an anxious attitude is problematic as it contributes to a vicious cycle with insomnia creating more fear and anxiety of going to bed, doubts about one’s ability to sleep, an unhealthy sleep routine and behaviours that are not recommended for sleep hygiene, more sleeplessness, more sleep worries about not sleeping, and on and on.
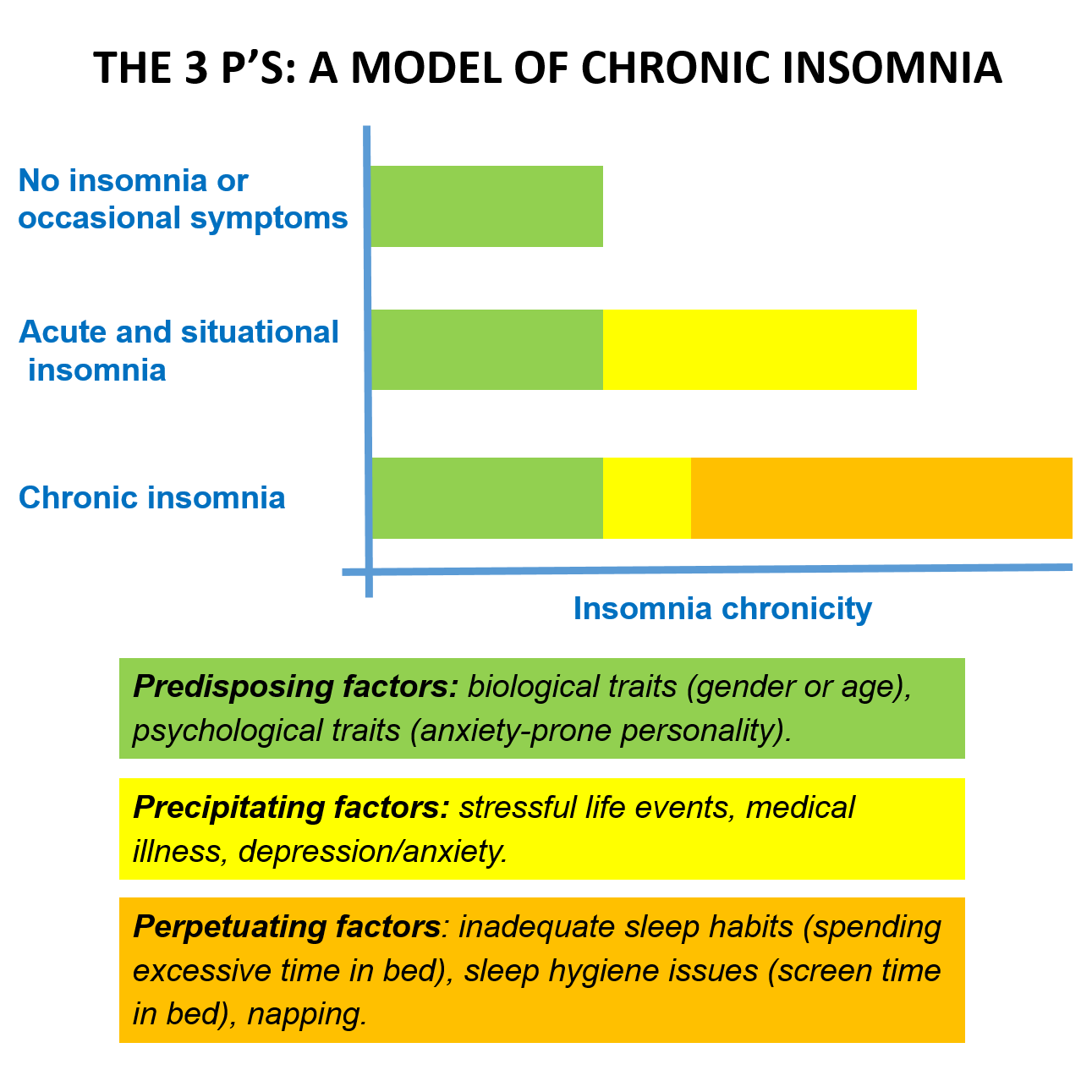
Since chronic insomnia is strongly related to our sleep dissatisfaction and erroneous beliefs about it, the key to change lies within our self and how we think and act about sleep. Before acting on our vicious cycle inducing thoughts/behaviours or taking medication (prescribed, over-the-counter or self-medication such as cannabis or alcohol use), the cause of insomnia symptoms must be ascertained with a healthcare provider who is knowledgeable about sleep (physician, psychologist, pharmacist, lung and airway specialist, etc.) See next section for more on the causes and factors that trigger and perpetuate insomnia.
If your insomnia symptoms are occasional or linked to an emotionally loaded transitional period, to help ease this over time, remember to maintain a healthy sleep routine and hygiene to not fall into the vicious cycle of insomnia.
For example, stick to a regular sleep schedule (same bedtime and wake time) as much as possible so you don’t aggravate your daily symptoms, and do not overuse sleeping aids such as pills and alcohol to help you fall asleep, as they can reduce the recuperative function of your sleep (less slow-wave sleep) and create addiction. Bet on healthier choices and stress management: exercise during the day, take in as much sunlight or the equivalent as possible, eat well, talk about what’s on your mind and clear your head as much as possible before going to bed. Try to maintain a comforting sleep routine and maybe add relaxation techniques to it such as deep breathing prior to sleep. Talking about insomnia symptoms with your physician or psychologist may also help you cope with the underlying stressful situation and get situational help and short-term treatment.
However, if you experience symptoms several times a week and for as long as three months, your insomnia symptoms are considered chronic, and you should not hesitate to talk about it with your physician or psychologist as they are the ones who can help. Unfortunately, sleep disorders including insomnia are not yet well known by many healthcare practitioners. Most of them will rely on medication such as sleeping pills, in an attempt to help ease your sleep. However, for chronic insomnia, this is not the treatment of choice. That’s because it can only have a very short-term effect since we adapt to the effects of this type of medication, which necessitate higher dosages for example. Moreover, sleeping pills can even aggravate your condition since these medications can reduce slow-wave sleep, the type of sleep that helps us recuperate, and it may lead to addiction.
When in doubt, it is always good to count on a sleep clinic or a healthcare provider who is knowledgeable about sleep to get accurate information and diagnosis and the best therapeutic options.